Follow
Follow
WEST HILLS
818-888-7878
ENCINO
818-986-1200
Home
Our Doctors
Alen N. Cohen, MD, FACS, FARS
Bob B. Armin, MD
Vera D. Cecilio, MD
ENT Services
Common ENT Problems
Adult & Pediatric ENT
Ear & Balance Disorders
Voice & Swallowing Disorders
Snoring & Sleep Apnea Surgery
Thyroid & Parathyroid Surgery
Head & Neck Surgery
Nose & Sinus
Allergy Management
Functional Endoscopic Sinus Surgery (FESS)
In-Office Balloon Sinuplasty
In-Office Turbinate Reduction
Nasal Fracture Repair
Nasal Polyp Surgery
Rhinoplasty/Nose Job
Septoplasty/Deviated Septum Repair
Cosmetics
Face
Common Questions
Facelift
Minilift
Necklift
Nose
Eyes
Botox/Dysport/Xeomin
Dermal Fillers
Non-invasive
Liquid Facelift
Fractionated CO2 laser resurfacing
Facial Reconstruction
Nasal Fracture Repair
Facial Fracture Repair
Skin Cancer
Otoplasty
Resources
Information Guides
Blog
A Guide On Thyroid Surgery
Your Guide to Sleep Apnea
Patient Forms
Contact
Encino Office
West Hills Office
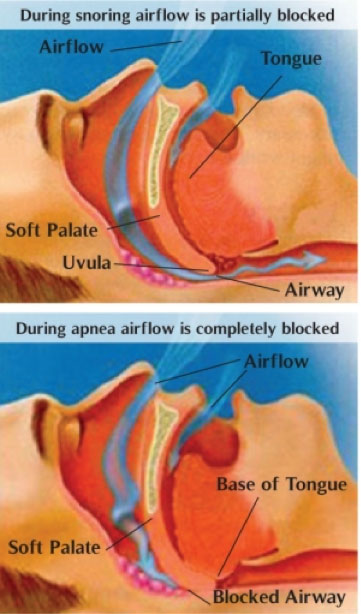
Sleep Apnea Graphic Helps You Understand What is Happening
About Us
Sitemap
Our Blog
Free Ebook
Privacy Policy
Patient Forms